August 09, 2021
Overview
Intravenous (IV) Cannulation is a technique in which a cannula is placed inside a vein to provide access for the administration of fluids, medications, contrast and blood products. It is one of the most common procedures completed within the Emergency Department.
Alignment to Western Health Best Care Framework
Right Care & Person-Centred Care
Why is this important?
The insertion of an IVC is a common clinical procedure in Western Health Emergency Departments. However, there are possible adverse outcomes associated with IVCs. The potential adverse outcomes associated with IVCs include pain, discomfort and most significantly the development of Hospital Acquired Infections (HAIs).
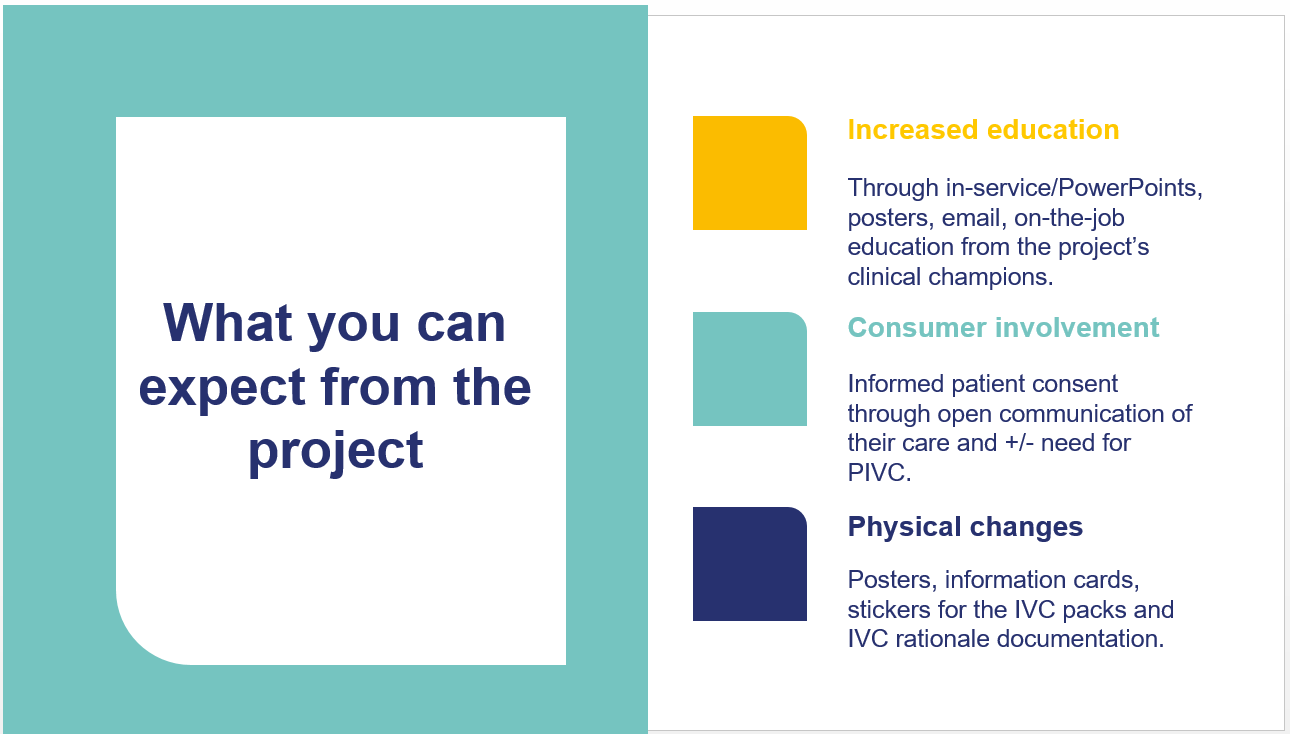
What does it look like in practice?
- Assessing the need/indication for an IVC.
- Selecting the right insertion site and appropriate size IVC.
- Inserting the device using aseptic technique and ensuring it is secured with a sterile semi-permeable dressing, such as the IV Frame Dressing.
- Documenting the insertion, maintenance and removal of an IVC on both the nursing chart and on EMR.
- Routinely inspecting the IVC insertion site and documenting the phlebitis score once a shift when accessing the device and if the patient expresses concerns.
- Assessing IVC patency by flushing the device at least once a shift.
- Reviewing the ongoing need for an IVC.
- Removing all IVCs that have not been inserted under emergency within 72 hrs.
- Remembering to remove all IVCs that have been inserted under emergency (including those inserted by AV) within 24 hrs.
Performance
- Quarterly Infection Prevention Audits on the Management of Invasive Devices and Aseptic Technique Audit Tool.
- Riskman pertaining to adverse complications, such as extravasation.
Policies, Procedures and Guidelines
OP-GC3 Peripheral Intravenous Cannulation
QRG’s
IVC QRG
Clinical Practice Links
Infection risks associated with peripheral vascular catheters; Journal of Infection Prevention
Webinar
#gallery-1 {
margin: auto;
}
#gallery-1 .gallery-item {
float: left;
margin-top: 10px;
text-align: center;
width: 33%;
}
#gallery-1 img {
border: 2px solid #cfcfcf;
}
#gallery-1 .gallery-caption {
margin-left: 0;
}
/* see gallery_shortcode() in wp-includes/media.php */
 Open Menu
Close Menu
Open search
Open Menu
Close Menu
Open search